Recommended Terms
Isoproterenol only increases heart rate, not blood pressure — suitable for patients with normal blood pressure but slow heart rate; if it slows further causing oxygen exchange problems, this drug is used to raise heart rate without raising blood pressure and causing hypertension symptoms.
Norepinephrine increases blood pressure but not heart rate — for example, in shock causing inadequate perfusion, when cardiac function is still normal but blood pressure has dropped, the goal is to raise blood pressure without stimulating the heart.
Epinephrine increases both heart rate and blood pressure — used in cases near death when both heart rate and blood pressure drop, for resuscitation.
Original Link
http://surg.dxy.cn/article/742522
Main Text
Epinephrine, Norepinephrine, Isoproterenol — Understand in One Article!
Previously on the forum, there was a case report:
Case Details
During the afternoon shift handover in a certain department, patient in bed 19 suddenly experienced respiratory and cardiac arrest! A group of people immediately began resuscitation, and Dr. L gave a verbal order: “two doses of ‘Adrenaline’ intravenous injection!”
The young nurse A involved in medication administration suddenly got confused about whether “Adrenaline” meant epinephrine hydrochloride or norepinephrine, but in panic did not forget to confirm with the doctor: “Is it norepinephrine, two doses?”
Dr. L replied with a casual “Mm” while performing chest compressions (none of the other rescuers noticed). Nurse A immediately injected norepinephrine for the patient, and the outcome can be imagined…
In fact, whether norepinephrine, isoproterenol, or epinephrine, they all belong to adrenergic receptor agonists, which bind to adrenergic receptors producing effects similar to epinephrine, thus also called sympathomimetic drugs.
Although in the same category, their clinical applications differ greatly. Today, let’s explore the differences and uses of these sympathomimetic drugs.
01 Different Chemical Structures
The basic chemical structure of sympathomimetics is β-phenylethylamine (Figure 1). When the hydrogens on the benzene ring carbons and the terminal amino group are replaced by different groups, various synthetic adrenergic receptor agonists can be created. These groups affect the drug’s affinity and stimulatory ability on α and β receptors.
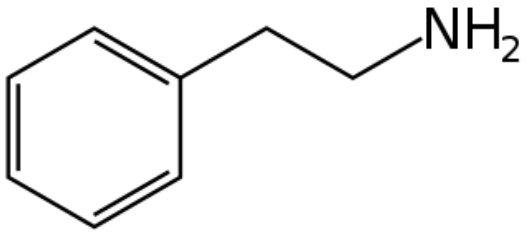
Figure 1. Phenylethylamine Chemical Structure
Epinephrine is mainly secreted by the adrenal gland. Its synthesis in the body is as follows: chromaffin cells (mainly in the adrenal medulla) use a series of catalytic enzymes to synthesize epinephrine from tyrosine (Tyrosine → DOPA → Dopamine → Norepinephrine → Epinephrine, process shown in Figure 2).
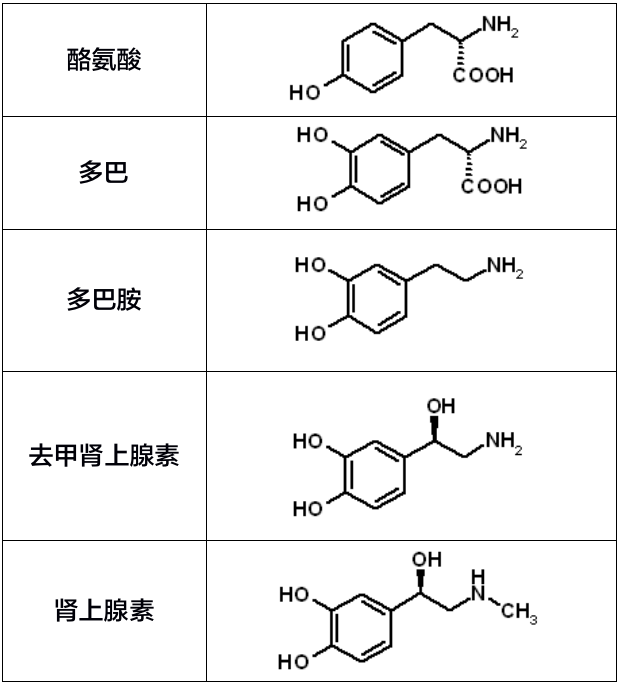
Figure 2. Epinephrine Synthesis in the Body
Epinephrine, norepinephrine, isoproterenol, and dopamine have hydroxyl groups on the 3rd and 4th carbons of the benzene ring, forming catechol, thus are called catecholamines.
Chemically, the difference between epinephrine and norepinephrine is that norepinephrine lacks a methyl group on the nitrogen atom; they were formerly called “adrenaline” and “noradrenaline” respectively.
Isoproterenol, compared to norepinephrine and epinephrine, is a synthetic product; its chemical structure is norepinephrine with the hydrogen on the amino group replaced by an isopropyl group, and it is a classic β1 and β2 receptor agonist.
02 Distinguishing Pharmacological Effects
✦ Norepinephrine:
Strong α receptor agonist, non-selective for α1 and α2, weak action on cardiac β1 receptors, mainly causes contraction of vascular smooth muscle, most evident in skin and mucosal vessels, followed by renal vessels, leading to increased blood pressure.
Small doses raise systolic pressure with little rise in diastolic pressure, increasing pulse pressure; larger doses raise both systolic and diastolic pressure with decreased pulse pressure.
✦ Epinephrine:
Agonist of both α and β receptors; acts on α1 receptors on vascular smooth muscle causing vasoconstriction (mainly skin, mucosa, renal vessels); and stimulates β2 receptors causing vasodilation (mainly skeletal muscle, liver, coronary vessels); also acts on β receptors in myocardium, sinoatrial node, and conduction system, strengthening myocardial contraction, increasing heart rate, accelerating conduction, and enhancing cardiac output.
Generally, subcutaneous or low-dose intravenous injection increases systolic pressure and decreases diastolic pressure; at higher intravenous doses both systolic and diastolic pressure rise significantly.
✦ Isoproterenol:
A β receptor agonist with low selectivity between β1 and β2.
Stimulates β1 receptors causing positive inotropic and chronotropic effects on myocardium, conduction, and rate, stronger than epinephrine; stimulates β2 receptors on vascular smooth muscle (skeletal muscle, liver, coronary vessels), causing vasodilation.
Because of cardiac excitation and peripheral vasodilation, usually increases systolic pressure, decreases diastolic pressure, with increased pulse pressure.
03 Clinical Applications to Remember
Table 1. Classification, Representative Drugs, and Indications of Sympathomimetic Drugs

✦ Norepinephrine
Common indications: Hypotension, shock.
Usage: Weight (kg) × 0.3 mg diluted into 50 mL of 5% glucose solution, 1 mL/h equals 0.1 ug/kg/min. To reduce local irritation, central venous infusion is recommended.
Typical dose: 0.05–0.4 ug/kg/min intravenous micro infusion, increase dose if necessary.
Precautions: Extravasation can cause local tissue necrosis; direct intravenous bolus leads to unstable blood pressure; avoid direct IV push.
✦ Epinephrine
Common indications: Cardiac arrest, allergic diseases.
Usage and dosage: For cardiac arrest patients, usually use undiluted epinephrine, 1 mg IV injection every 3–5 minutes; for severe allergic reactions, recommended intramuscular injection of undiluted epinephrine (1:1000), 0.01 mg/kg (max 0.5 mg).
Precautions: Usage varies by indication. After peripheral IV bolus, flush with saline to ensure drug reaches the heart. (See details at Epinephrine cannot be “directly IV pushed”? Guidelines on use in cardiac arrest)
✦ Isoproterenol
Common indications: Sick sinus syndrome, severe or third-degree atrioventricular block causing bradycardia.
Usage: 1 mg isoproterenol diluted into 50 mL normal saline.
Typical dose: 2.0–20 μg/min, usually effective at 2–4 μg/min.
Precautions: Increases myocardial oxygen consumption and decreases perfusion pressure, so use cautiously in coronary artery disease patients.
Planner | Li Ya
First published | Cardiovascular Times
Clinically, besides paying attention to drug compatibility, it is also important to watch for conflicts with drug co-administration.
Indeed, even the best drugs have their limitations; rational drug use maximizes benefits. The “Rational Medication” feature in the Medication Assistant App greatly helps doctors solve clinical medication problems.
The “Medication Assistant – Rational Medication” was developed by professionals and provides rational usage instructions for each drug ingredient, including four modules: “Indications and Dosage, Safe Use, Pharmacology and Toxicology, Patient Education.” Content is compiled from the latest authoritative information including drug labels, guidelines, and literature, reviewed and updated by over a hundred experts in real-time, offering comprehensive clinical medication decision support to doctors.
**\\u003e\\u003eClick here to jump to “Rational Medication”**

Copyright Statement
All text, images, and audio/video materials on this website labeled “Source: Dxy.cn” are copyrighted by Dxy.cn. Without authorization, no media, website, or individual may reproduce them. Authorization must cite “Source: Dxy.cn.” All reprinted articles here are for disseminating more information and clearly state the source and author; media or individuals not wishing their content reprinted may contact us for immediate removal. Reprinted content does not represent the views of this site.