This article was transcoded by SimpRead, original address m.medsci.cn
Dear friends, during director ward rounds, imaging department rotations, resident exams, or job interviews, have you ever encountered such a question? Explain the MRI evolution of cerebral hemorrhage. At that moment, do you feel secretly pleased, or only awkwardly familiar?
Dear friends, during director ward rounds, imaging department rotations, resident exams, or job interviews, have you ever encountered such a question? Explain the MRI evolution of cerebral hemorrhage. At that moment, do you feel secretly pleased, or only awkwardly familiar?
If you can’t remember it, you really can’t blame yourselves. Who’s brave enough to boldly counter-question their superior once? I estimate that at least half the time, they wouldn’t answer well either. Why is this so hard to memorize? I think there are several reasons: 1. Textbooks differ, and one teacher’s explanation is not the same as another’s, so which one should you memorize? You memorize one version in college, one version when you start working, then after a few years another version appears in an imaging book—are they just playing games with us? 2. The changes are varied and rules unclear; those fluctuating high and low signals over hours and days are confusing and maddening. At our age, it’s no longer prime time for rote memory; without full understanding, you truly can’t remember anything. 3. It’s rarely used in practice. In emergencies, a patient comes with headache or hemiplegia; a quick head CT shows cerebral hemorrhage, then continues with CT follow-up, making all our painstaking memorized knowledge useless.
I. First, solve the first problem. After extensive searching and referencing multiple Chinese and English sources, comprehensively considering scientific accuracy, consistency, and memorability, I strongly recommend the following table.
Three major advantages:
-
Temporal regularity: 1, 3, 7, 14 days—just these clear time points, unlike some textbooks that confuse with hours, days, then weeks, making it bewildering.
-
Clear signals, unlike many places with fluctuating isointense, hyperintense, or hypointense signals that are too detailed and useless to memorize.
-
Concise interpretation of hematoma component evolution, facilitating further understanding for interested students.
![]()
P.S. Of course, temporal and signal changes in practice aren’t absolute; this primarily shows arterial-source hemorrhage manifestations. Hematoma size, composition (what about venous source?), location, rebleeding, communication with subarachnoid space/ventricles, and sequence variations among hospitals also affect signals significantly. Therefore, just mastering one reliable table lets you adapt and extrapolate flexibly.
II. Next, solve the second problem by analyzing the table content.
Starting with the easy part: right after arterial bleeding, red blood cells are intact and contain oxyhemoglobin—this is the hyperacute phase, the most original state. After one day, red blood cells remain intact but oxygen is lost; hemoglobin becomes deoxyhemoglobin—this is the acute phase. Two days later, red blood cells still intact, but deoxyhemoglobin is oxidized to methemoglobin—this is the early subacute phase. After a week, red blood cells finally rupture and break down; methemoglobin is released freely, a hallmark of the late subacute phase. Finally, in the chronic phase, hemosiderin is deposited after ferritin and methemoglobin transformation, which can be seen for years.
Alas, it’s hard to clearly explain these two paragraphs in a short space. Those uninterested can skip ahead. First, three concepts: diamagnetic, paramagnetic, and superparamagnetic, related to the number of unpaired electrons in iron atoms. Clinicians don’t delve so deep; just remember oxyhemoglobin is diamagnetic, deoxyhemoglobin and methemoglobin are paramagnetic, and hemosiderin is superparamagnetic. Although deoxyhemoglobin and methemoglobin are both paramagnetic, the iron atom’s position within the hemoglobin framework affects MRI signals differently.
Let’s examine each phase:
-
Hyperacute phase: oxyhemoglobin within red blood cells; oxyhemoglobin is diamagnetic. The hematoma affects MRI mainly because it contains a lot of water, thus T1 shows low signal, T2 shows high signal (similar to usual edema).
-
Acute phase: two factors influence signals—first, deoxyhemoglobin is paramagnetic, which influences T2 making it darker; second, the deoxyhemoglobin structure limits effects on T1, which remains dark. Therefore, this is the darkest phase with both T1 and T2 appearing black.
-
Methemoglobin phase: still paramagnetic, T2 remains dark, but T1 turns bright due to changes in iron atom location in methemoglobin compared to deoxyhemoglobin.
-
When the cellular membrane ruptures, paramagnetic effects on T2 wane, water content in hematoma rises, and T2 becomes brighter; this “double bright” phase is the easiest cerebral hemorrhage stage to remember.
-
Chronic phase: hemosiderin is water-insoluble and superparamagnetic, so both T1 and T2 are dark. If this section is hard to understand or remember, it’s okay; just memorizing the table won’t affect clinical application. Interested readers can check the references for details.
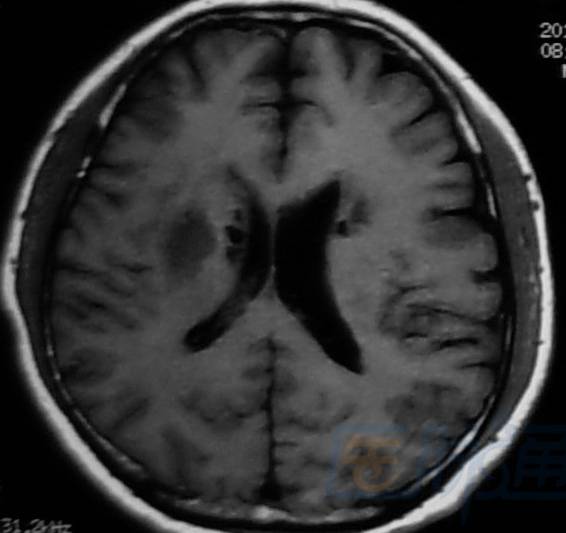
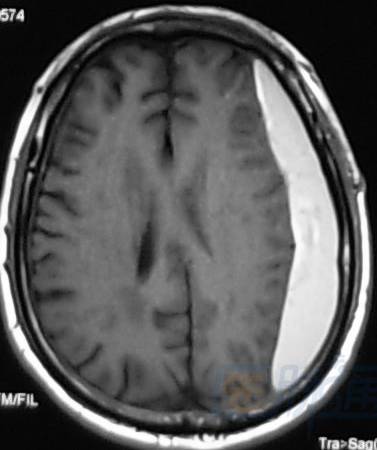
Now solve the third problem; let’s relax with images to consolidate today’s learning, showing T1 first, then T2.
Hyperacute phase (<24h): next to right ventricle
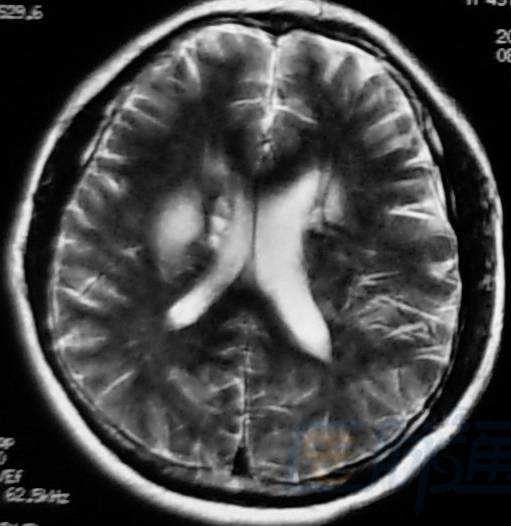
Acute phase (1–3 days): right occipital lobe
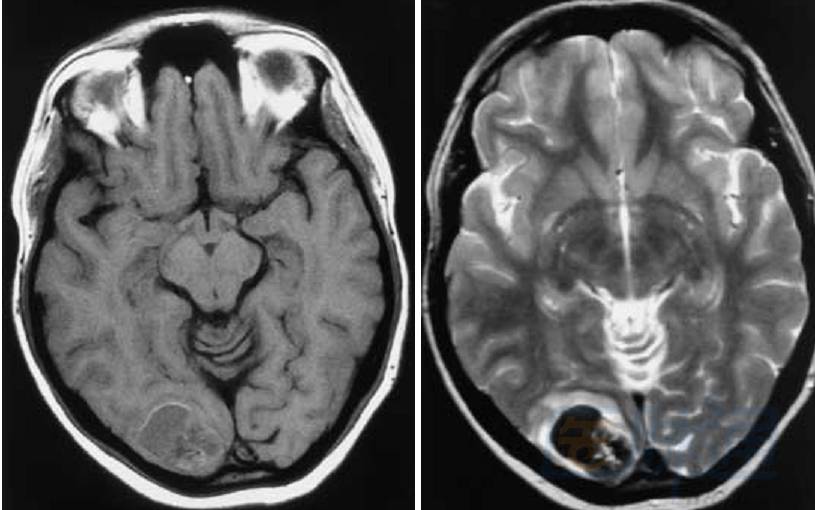
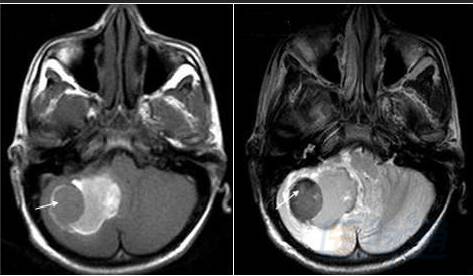
Early subacute phase (3–7 days): pons

Late subacute phase (7–14 days): left subdural
![]()
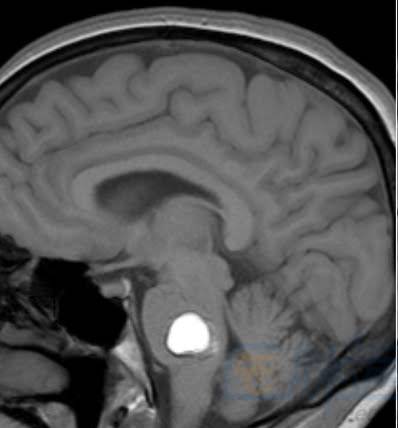
Chronic phase (>14 days): arrow
Finally, an honest truth: can you memorize this in ten minutes? Of course not, human brains aren’t USB drives into which you just copy stuff. If you review for ten minutes today, retaining even 30% tomorrow is quite good. You must review repeatedly after several days, then repeat again; without five or ten ten-minute sessions you definitely won’t remember (smart friends please don’t shoot me). Also, don’t just blindly memorize. When encountering cerebral hemorrhage MRI in clinic, immediately bring up and practice against the table, ideally take pictures for archiving and reinforcement later, so you can feel the joy. Here’s another tip: if difficult to memorize, take it step-by-step—first consider hyperacute phase as ordinary edema, memorize the characteristic “double bright” late subacute phase, then memorize the “double black” acute and chronic phases, and finally learn the hard-to-remember early subacute phase. By the way, both T1 and T2 have two bright and three dark stages—isn’t that interesting?
That’s it for today. Digest traditional T1 and T2 for a few days; then we’ll cover trendier sequences that actually change guidelines, namely GRE gradient echo, and the relatively newer DWI and FLAIR sequences compared to T1 and T2. A personal thought—what era is this that T1 and T2 are still tested? That’s so low-tech. Nowadays, even if not everyone has GRE (and T2*, SWI, aren’t those confusingly similar?), everyone should at least have DWI and FLAIR, according to practical principles.
Source: Radiology Salon
Copyright Statement:
All content marked as “Source: MedSci” or “Source: MedSci Original,” including text, images, and audio-video materials, are copyrighted by MedSci. Without authorization, no media, website, or individual may reproduce them. Authorized reproductions must indicate “Source: MedSci.” All reprinted articles are for disseminating more information with clear source and author attribution. Media or individuals objecting to reprints may contact us for immediate removal. Reprinted content does not represent the position of this site.
Leave a message here
Blockquote